
Chest pain—it’s one of the most common yet terrifying complaints in medicine. Is it a heart attack? Acid reflux? A pulled muscle? As clinicians, we need a systematic, foolproof approach to avoid missing life-threatening causes while not over-investigating benign ones.
In this guide, I’ll break down the key causes of chest pain, the must-do workup, and some clinical pearls. Plus, I’ve got a free downloadable sketch (linked below) to help you visualize this.
Why Chest Pain Scares Us (And Rightly So!)
Chest pain can signal anything from GERD to a massive MI or aortic dissection. Missing the bad stuff can be deadly, but over-testing isn’t great either. So, how do we strike the balance?
Spoiler: It’s all about pattern recognition + smart testing.
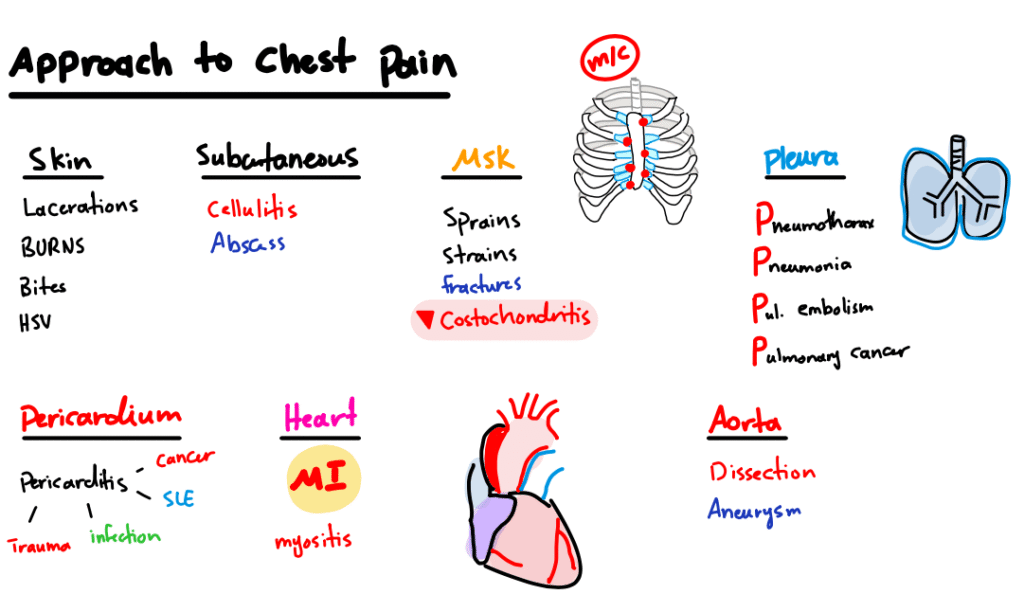
The Big Categories of Chest Pain
Let’s categorize chest pain based on anatomy—because that’s how our brains work best.
1. Skin & Subcutaneous (The “Oh, That’s Why It Hurts” Causes)
- Lacerations, Abscesses – If the patient says, “Doc, I got stabbed,” well… yeah.
- Burns & Bites – Hot coffee spills, spider bites, or even HSV (yes, shingles can mimic cardiac pain!).
- Costochondritis – That tender spot when you press on their sternum? Bingo.
🔹 Clinical Pearl: If pressing on the chest reproduces pain, think MSK (musculoskeletal) first.
2. Pericardium (The “Is This My Heart?” Zone)
- Pericarditis – Sharp, pleuritic pain relieved by leaning forward. Look for diffuse ST elevations on EKG.
- Malignancy/Infection – Rare but sneaky.
🔹 Workup: EKG, echo if suspicious.
3. Esophagus (The “Heartburn or Heart Attack?” Dilemma)
- GERD – Classic retrosternal burning, worse after eating.
- Esophagitis/Perforation – If they’ve been vomiting violently or swallowed something sharp, think Boerhaave’s syndrome.
🔹 Test: Trial of PPIs, maybe an endoscopy if red flags.
4. Chest Wall & Muscles (The “I Lifted Weights Yesterday” Group)
- Strains, Fractures – Trauma? Rib fractures are a thing.
- Myositis – Inflamed muscles = pain with movement.
🔹 Pearl: If pain changes with position or palpation, it’s likely not cardiac.
5. Lungs (The “Breathing Hurts” Causes)
- Pneumothorax – Sudden, sharp, with SOB.
- Pneumonia/PE – Pleuritic pain, cough, hypoxia.
- Pulmonary Cancer – Chronic, worsening pain.
🔹 Workup: CXR, EKG, D-dimer (if PE suspected), CT if needed.
6. Aorta (The “Oh Sh*t” Category)🚨
- Aortic Dissection – Tearing pain, radiating to back, unequal BPs.
- Aneurysm – Less acute but still dangerous.
🔹 Test: CTA or MRI STAT.
7. Cardiac (The “Don’t Miss This” Group)
- MI – Crushing, radiates to arm/jaw, + sweating/nausea.
- Angina – Exertional, relieved by rest/nitrates.
🔹 Workup: Troponins, EKG, maybe cath lab.
The 3 Must-Do Tests in Every Chest Pain Workup
1️⃣ Chest X-ray – Rules out pneumothorax, pneumonia, rib fractures.
2️⃣ 12-Lead EKG – Looking for STEMI, pericarditis, arrhythmias.
3️⃣ Troponins – If cardiac ischemia is a concern.
Bonus: If dissection is suspected, CTA aorta. If PE, CTPA or V/Q scan.
Quick Clinical Pearls
✔ Reproducible pain? Likely MSK or GERD.
✔ Pleuritic pain? Think PE, pneumothorax, pericarditis.
✔ Tearing + back pain? Aortic dissection until proven otherwise.
✔ Relieved by nitroglycerin? Probably cardiac.
Free Downloadable Sketch 📝
To make this even easier, I’ve created a simple, visual guide summarizing this approach. Grab it here 🔗
Final Thoughts 💜
Chest pain is a bread-and-butter complaint, but it demands respect. Use a structured approach, trust your clinical instinct, and don’t hesitate to escalate if something feels off.
Got questions? Drop them below—I’ll answer!
And if you want a deeper dive, check out my YouTube lecture on this topic 🔗